60 M acute coronary hypotension
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box is welcome."I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.























I am presenting a case of 60 year old man who came to the OPD with
Chief complaints :-
Abdominal pain since 10 days
History of presenting illness :-
The patient was apparently asymptomatic 10 days ago then he developed abdominal pain which is dull aching type, non radiating, no aggravating and relieving factors.
The patient also has a history of hematuria which subsided now and poor stream of urine.
No h/o - vomiting
No h/o - fever and chills
No h/o - trauma
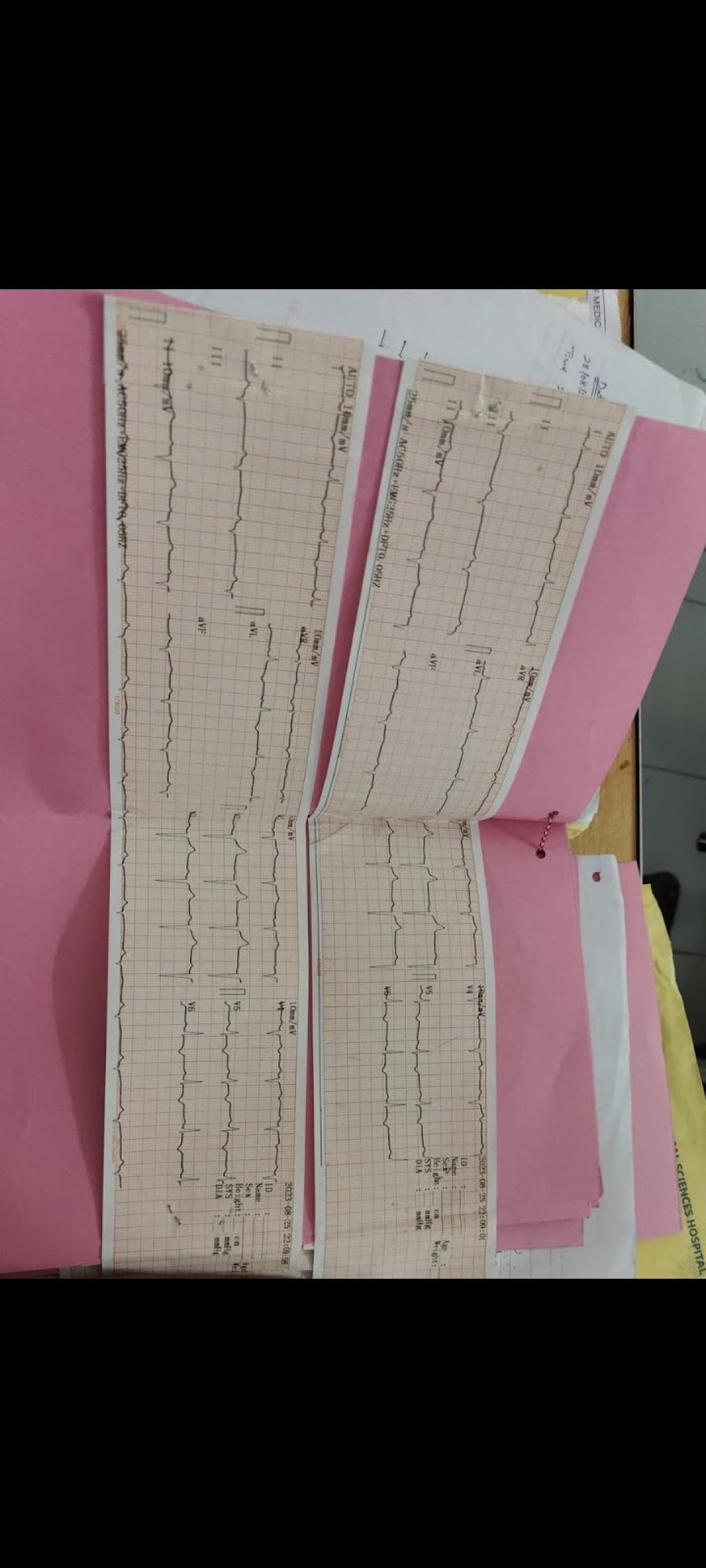
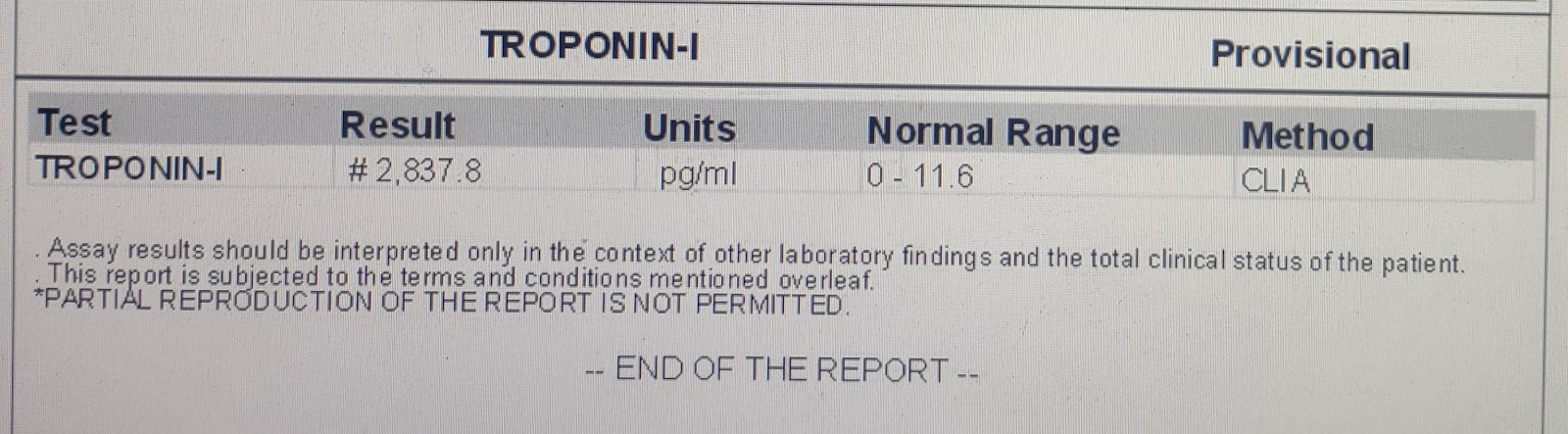
Pod 0 patient developed hypotension and genral medicine referral was taken and patient was diagnosed ?nstemi an ECG showed t wave inversion AVL lead1 v 5,V6 Pt was admitted in ICU .
After admission in ICU the patient was started started on dobutamine (6ml/hr) on 26/08/23 and on 27/08/23 noradrenaline(5ml/hr) was also given along with dobutamine (2ml/hr) later that day dobutamine was discontinued and on 28/08/23 the patient was only on noradrenaline (3ml/hr) . On 29/08/23 the patient was discontinued of noradrenaline and dobutamine was started (3ml/hr) . On 30/08/23 the patient was still on dobutamine (2ml / hr ).
Past history -
K/c/o - DM since 2 yrs ( on medication METFORMIN - 500 mg PO / OD ).
N/k/c/o HTN / BA / epilepsy .
Surgical history -
Surgery was done on July 2022 for bilateral ureteric calculus and bladder calculus ( URSL + cystolithotripsy + Dj stenting) .
Personal history :-
Diet :- Mixed
Appetite :- normal
Sleep :- Adequate
Bowel and bladder :- regular
No addictions
No drug or food allergies.
General examination :-
Patient was concious coherent cooperative .
Moderately build and nourished.
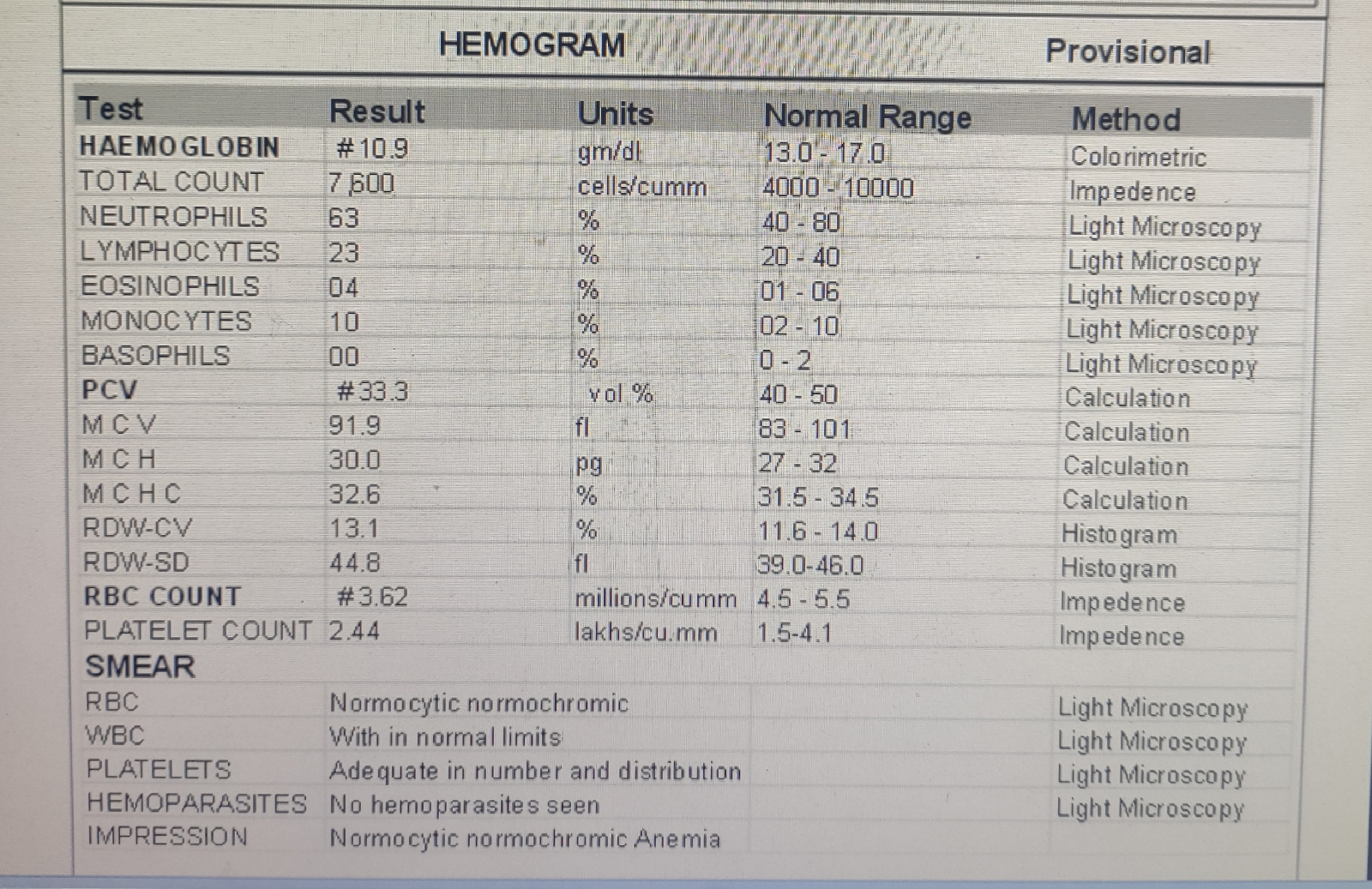
Pallor- present
Icterus - absent
Cyanosis - absent
Clubbing - absent
Lymphadenopathy - absent
Edema- absent
Vitals :-
Temperature – Afebrile ( 98.6 F )
Pulse rate – 65 bpm , regular
Respiratory rate – 16 cpm
BP - 90/70 mmhg
Spo2 - 97 on room air
GRBS - 180 mg / dl
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
INSPECTION :-
Chest is elliptical shaped, bilaterally symmetrical.
Trachea appears to be central
Movements are equal bilaterally.
No scars or sinuses
Apical impulse seen in 5th intercostal space lateral to midclavicular line.
PALPATION :-
All the inspectory findings are confirmed
Trachea is central
Apical impulse felt at 5th intercostal space lateral to midclavicular line.
AUSCULTATION :-
S1 S2 heard no murmurs .
RESPIRATORY SYSTEM
INSPECTION :-
Elliptical.
bilateral symmetrical.
Trachea is central
Movements are equal bilaterally
Visible epigastric pulsations
No scars or sinuses
Apical impulse not seen.
PALPATION :-
All inspectory findings are confirmed: Trachea is central, movements equal bilaterally.
Apex beat felt in left 5 th intercoastal space.
PERCUSSION :-
Resonant note heard in all areas bilaterally
AUSCULTATION:-
Bilateral air entry present – Normal vesicular breath sounds heard.
PER ABDOMEN
INSPECTION
Shape of abdomen appears to be Normal
No Visible epigatric veins
No engorged veins sinus scars
PALPATION
All inspectory findings conformed
Abdomen soft & Non tender
No organomegaly
PERCUSSION
Tympanic note heard all quadrants abdomen
AUSCULTATION
Bowel sounds heard.
CENTRAL NERVOUS SYSTEM :-
HMF - Intact
Speech – Normal
Motor and sensory system – Normal
Reflexes – Normal
Cranial Nerves – Intact
Gait – Normal
Cerebellum – Normal
Clinical images :-
Investigations :-
On 24/08/23 :-
On 25/08/23:-
On 26/08/23 :-
At 1.00 am
At 3.00am
At 7.00am
On 27/08/23:-
On 28/08/23
On 29/08/23
On30/08/23
Comments
Post a Comment